While male and female bladder anatomical models usually display the exact same bladder organ itself, they differ significantly in their surrounding pelvic organs and urethral structures. These variations completely alter the overall layout and proportions of the models.

Key Differences:
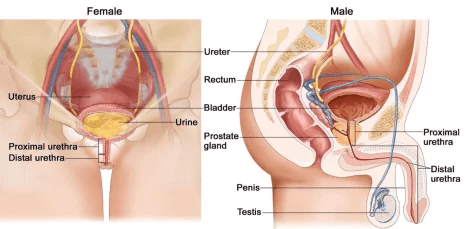
- In the male model, the bladder is positioned above the prostate gland and anterior to the rectum.
- In the female model, the bladder is located anterior to the vagina and inferior to the uterus.
- The male urethra is much longer than the female urethra, so male models typically show a longer exit pathway from the bladder to the external orifice.
- Female models demonstrate a more compact bladder-to-urethra arrangement due to the shorter female urethral tract.
- The detrusor muscle in males is often depicted as thicker than in females, reflecting the different voiding mechanics required by a longer male urethra.
Why Are Male and Female Bladder Models Different?
| Feature | Male Bladder Model | Female Bladder Model |
| Bladder Position | Above the prostate | In front of the vagina and uterus |
| Urethra Length | Approximately 18–20 cm | Approximately 3–5 cm |
| Prostate | Included | Not present |
| Reproductive Organs | Prostate, seminal vesicles, vas deferens | Uterus, cervix, vagina (depending on model) |
| Catheterization Training | More challenging (due to length and curves) | Easier and shorter pathway |
| Common Teaching Topics | BPH, prostate surgery, urinary retention | Female catheterization, pelvic anatomy, pregnancy-related anatomy |
1. Urethral Length and Pathway Dynamics
The most prominent anatomical distinction between these two models lies in the urethra, which directly dictates how urinary catheterization is taught.
Male Bladder Model: Its urethral pathway is significantly longer (typically 18–20 cm in real life). The model must accurately depict three distinct segments: the prostatic urethra (passing through the prostate), the membranous urethra, and the spongy/penile urethra. It also displays the natural “S-shaped” curve, which is vital for training students on how to avoid urethral trauma during catheter insertion.
Female Bladder Model: Displays a short, straight urethral tube (approximately 3–4 cm). This model highlights the close proximity of the urethra to the anterior vaginal wall, visually demonstrating why female patients face a significantly higher clinical risk for Urinary Tract Infections (UTIs) than males.
2. Surrounding Reproductive Organ Integration
A high-quality bladder model does not exist in isolation; it must showcase the exact spatial relationships with neighboring pelvic organs.
Male Model Configuration: Advanced male bladder models explicitly integrate the prostate gland encircling the bladder neck, alongside the seminal vesicles and the vas deferens. This layout is indispensable for urologists and educators to explain Benign Prostatic Hyperplasia (BPH) or how an enlarged prostate compresses the bladder neck, leading to urinary retention.
Female Model Configuration: The female model highlights the bladder’s position directly anterior to the uterus and vagina. This structural layout is essential for demonstrating obstetric pressure during pregnancy, pelvic organ prolapse (cystocele), and how uterine fibroids can compress the bladder wall.
3. Trigonum Vesicae (Bladder Trigone) and Muscular Walls
While both models feature the internal Trigonum Vesicae (the smooth triangular region at the bladder base formed by the two ureteric orifices and the internal urethral orifice), their structural surroundings differ:
- The Detrusor Muscle Layer: High-precision sectional models display the thick muscle tissue constituting the detrusor wall. In male models, this muscular wall is typically rendered with more pronounced trabeculation (thickening) to visually represent how the bladder works harder to pump urine against potential prostate obstructions.
- Sphincter Mechanics: The male model clearly isolates the powerful internal urethral sphincter at the bladder neck, which prevents retrograde ejaculation—a feature structurally distinct from the female pelvic floor sphincter network.
What to Look for When Choosing a Bladder Anatomical Model
If you are sourcing bladder models for institutional or educational use, keep the following considerations in mind:
- Accuracy of Adjacent Organs: Ensure the male model accurately depicts the prostate and penis, while the female model correctly integrates the uterus, vagina, and ovaries.
- Level of Detail: High-quality teaching models should clearly separate the anatomical structures of the bladder wall, urethra, trigone, and sphincters.
- Intended Use Case: If the model is being used for practical urinary catheterization training or pelvic anatomy labs, the accuracy of the urethral length and relative pelvic spatial relationships are the most critical factors.